|
|
|
| Drinking water in the arid zone of western Rajasthan | |
|
Drinking Water Quality
Drinking water in the arid zone of western Rajasthan 1. Introduction 2. Traditional approaches to water use efficiency - water harvesting systems 3. Microbiological quality of harvested/stored water 4. Solar disinfection as a point-of-use water treatment system 5. Optimizing the solar disinfection procedure prior to field trials 6. Field study 8. Conclusions 10. References Rajasthan is the largest state in Exposure to waterborne infectious diseases is a significant issue in rural Traditional approaches to water use efficiency - rainwater harvesting systems For the same reason, if a woman should need to drink water directly from a nadi or talab, she will often use her headscarf veil (known locally as a "dupatta") or the edge of her sari to filter the water during drinking. However, apart from such simple filtration procedures, water is usually drunk straight from the source, without any treatment. This is partly due to a lack of awareness of the risks of transmission of disease via the water supply, but is also due to the absence of a suitable method of treatment. For example, fuelwood is scarce in the region, so very few people are able to boil their water before drinking, and the inconsistent availability of chlorine tablets (usually through the community health worker) for the treatment of water stored in tankas means that people cannot always rely on this approach. Similarly, while alum ("fitkari") can be used as a coagulant to treat highly turbid water in village community tankas, it is expensive and erratically available (often, only in cities and larger towns). As a result, such untreated supplies represent a potential means of transmission of waterborne infectious diseases, including dysentery, cholera and gastroenteritis, which are not removed by the traditional filtration procedures described above. In our routine testing of such waters using field kits for H2S-producing bacteria, we have found that almost all of the surface water and stored water supplies are grossly contaminated. Water is usually stored on a daily basis in traditional earthenware pitchers ("matkas"), where evaporation from the surface reduces the water temperature, making it more pleasant to drink in the hot climate. Thus villagers will often select water based on such behavioral patterns, for example from the coolest available source in summer, rather than considering the potential for waterborne disease. However, there is also a traditional belief that storage in pitchers made from either copper or brass helps improve the quality of the water, thereby reducing stomach upsets and aiding well-being. The microbiological basis for this has been confirmed by recent studies demonstrating that fecal coliform bacteria are inactivated by storage for 48 hours in a traditional copper and brass vessels (Tandon, Chhibber and Reed 2005). However, water is rarely stored for that long, being usually collected and consumed daily. In recent years, villagers have moved away from copper vessels, such as when they use plastic containers to transport water to school or work. This behavioral change may be driven by the ready availability of such plastic items; for example, discarded plastic mineral water bottles used by tourists are obtainable in villages near to highways. Additionally, plastic is lighter, less expensive than traditional metal pitchers, and may be seen as more "modern" than brass and copper vessels. In our studies in rural Rajasthan, we have found that while most of the villagers are aware of the traditional belief in the effectiveness of copper and brass pots, they do not make use of such metal pitchers for water storage, though a few make use of brass pitchers for collecting and carrying water to the household. Given the limited amount of safe water for drinking and the recent problems with drought conditions in western Rajasthan, we felt that it would be worthwhile to see whether solar disinfection might be a useful means of providing rural villagers with an alternative source of safe drinking water. The Wellcome Trust The use of sunlight is one of the oldest recorded methods of water purification in At its simplest ("batch-process" solar disinfection), the method involves filling a transparent plastic or glass vessel with contaminated water and then keeping this vessel in full-strength sunlight for several hours, to inactivate pathogenic microbes. Using discarded plastic (PET) drinks bottles in laboratory and field experiments, research has demonstrated that solar radiation can inactivate a wide range of microbes, including fecal indicator bacteria such as E. coli, waterborne pathogenic bacteria such as those responsible for cholera and dysentery, and certain viruses and protozoal parasites. Continuous-flow solar water treatment systems have also been developed and evaluated, though these are more complex and sophisticated in design and operation (for a more detailed review of solar water treatment, see Reed 2004). Solar disinfection is the result of two processes: It is generally accepted that optical inactivation due to solar UV radiation is the main component of solar disinfection. However, research has shown a synergistic interaction between optical and thermal inactivation at temperatures above 45°C (~113°F), where the combined optical and thermal effects act to inactivate bacteria at a faster rate than would be predicted from the effect of each factor in isolation (Reed 2004). Since the optical inactivation process involves the sunlight-driven production of reactive oxygen species, solar disinfection is strongly influenced by the level of dissolved oxygen in the water, being optimum only under oxygen-saturated conditions; however, this is relatively easily achieved by leaving a small air gap during filling, and then shaking the bottle (Reed 1997). The optical inactivation process is also sensitive to water turbidity, being most effective with water of low-to-moderate turbidity (typically up to100 turbidity units). For water of higher turbidity, a three-stage process can be used: 1. Clarification - by sedimentation, filtration or coagulation/flocculation (in Rajasthan, the villagers sometimes add dried sand, known locally as "balu mitti," to reduce the turbidity of water with a high level of suspended solids before use). Laboratory trials, have compared the effectiveness of bottles with transmissive, reflective and absorptive rear surfaces by adding a suspension of Escherichia coli to pre-sterilized distilled water. Our results have shown that while the black-backed bottles were the most effective in inactivating fecal indicator bacteria under full-strength sunlight, a reflective backing was best under sub-optimal sunlight conditions (cloudy skies) where the rate of solar disinfection was slowest, showing around 25% enhancement in the rate of inactivation under low sunlight conditions, compared to transmissive and absorptive rear surfaces. As a result of these experiments, we decided to evaluate the custom-made 1-liter bottles with stainless steel reflective backings under field conditions in western Rajasthan, since it is important to have the best rate of inactivation under sub-optimal light conditions. Field locations The villages of Tulesar Purohitan ,Tulesar Charan and Bambore Boarli lying within the rural interior of Jodhpur district approximately 30 km (~19 mi) east of Jodhpur city, were selected as suitable field locations to evaluate the household-level use of solar disinfection. Each village has a population of around 1500 persons. Tulesar Puohitan and Bambor are mainly composed of members of the Rajpurohit caste, a vegetarian community that maintains links with other ruling and religious groups such as the Brahmins, while Tulesar Charnan mostly comprises the Meghwal caste, a non-vegetarian occupational group engaged in tanning/weaving and similar manual activities. While each village has its own talab, both villages are connected by a pipeline that can provide safe, non-saline water from a borewell around 45 km (~28 mi) away. However, this pipeline also supplies 40 other villages along the route, and water is only available intermittently, due to frequent failures in the electricity supply and to lack of an adequate supply in the borewell. Typically, water is pumped to each village once every 10 days or so. In Tulesar Purohitan, the piped water is stored in a large village community tanka from where it is collected by bucket and rope, whereas in Tulesar Charnan the external supply is via a standpost and community tap on the edge of the village, which is supplemented by government water tanker every few days during the dry season. Regardless of the source, water is transported to the home in metal vessels, and then stored in earthenware matkas before drinking, especially in the summer months, when the surface water temperatures can exceed 50°C (~122°F). The lack of a consistent supply of safe groundwater means that both communities would benefit from an effective treatment system for their local surface water. The villagers of Tulesar Purohitan maintain and utilize their talab to a greater extent than the villagers of Tulesar Charnan, with appropriate religious rituals/observances that give due regard to its traditional role as a source of water; thus, cattle dung is regularly removed from the immediate vicinity of the talab, and anyone found urinating or defecating in the catchment area is charged 50 rupees (just over US $1) as a penalty. In Tulesar Charnan, the people prefer to use the external water supplies (public standpost or government tanker), and only use the talab water when these external supplies are unavailable. In both villages, animals are allowed free access to the talab, to drink and bathe, creating further contamination and increasing the turbidity of the water. We began our initial work in 2002, selecting families in each village for a year-long baseline study prior to the introduction of solar disinfection as part of a further year's follow-up study. However, the ongoing drought meant that all local talabs and nadis were dry, and the people were entirely reliant on additional supplies of clean water brought in by government tanker. The drought eased only in 2004, and a change in plan was required, due to the shortened timescale of the project: 40 families in each village were randomly assigned either to the treatment group, who were to use solar disinfection, or to the control group, who were to continue with their previous practices (20 families per group, with around 4 adults and 3 children per family). Each family in the treatment group received 12-15 custom-made 1-liter solar disinfection bottles and reflectors. Most of the families live in "pakka" (good quality) houses, soundly constructed with bricks and cement, with a tiled roof and a terrace, whereas the remainder are in "kachcha" (makeshift) houses, with clay walls and grass or brushwood roofs. Irrespective of the type of dwelling, all families had either a cemented terrace or a cleared area close to the dwelling where solar disinfection bottles could be kept in full sunlight for most of the day. In all families, the women and children are responsible for collection and storage of water. In contrast with some other areas of Evaluation of field trials Monthly surveys of the incidence of gastroenteritis/diarrhea were carried out, alongside testing of the local water supplies (all talab and tanka water was found to be highly contaminated on every test occasion, whereas the piped water supply tested negative for bacteria contamination). Despite the turbidity and color of the surface waters, solar experimental studies carried out in the laboratory at Kochi using E. coli added to pre-sterilized water samples showed that the rate of solar inactivation of fecal indicator bacteria in such waters was broadly equal to that of non-turbid distilled water to which the same strain of E. coli had been added. The families in the treatment group who were using solar disinfection to treat their drinking water reported substantially fewer incidences of gastroenteritis/diarrhea than the control group in both villages, with an overall reduction of around 70% across all seasons. There was also a widely held view among those in the treatment group that drinking solar treated water led to a greater sense of overall well-being and an enhanced ability to work, attend school, etc. In the later stages of the field trials, this view also spread to members of the control group, who felt a sense of exclusion since they had not been given the solar disinfection bottles. Implementation of solar disinfection began in January 2004, which is the cool season in Rajasthan. At such times, the ambient daytime temperature is typically 20-25°C (~68-77°F), and people prefer to drink warmer water; thus the solar treated water could be consumed at the end of a day's sunshine, and was consistent with the traditional preferences of the local people. As the temperature increased towards the annual maximum of around 42-45°C (~107.5-113°F) in May-June, the water had to be kept indoors overnight in order to reduce its temperature; this reduced its appeal to some of the families, who were intermittent in their use of the bottles. However, many of the villagers in the treatment groups were still positive about the use of the system, since they could appreciate that a closed bottle also blocked the access of flies and other insects to the treated water. Some families developed their own procedures to reduce the temperature of the water prior to consumption, for example by keeping the bottles overnight in a half-filled earthen matka. Individuals who took the bottles to work or school often covered them with cloth to prevent the water from overheating on the following day, while others cooled them in shaded ditches. A more significant drawback to the use of the solar water treatment bottles in summer was reported for those using unfiltered water directly from the talab; in such cases the treatment process gave the water a foul smell, presumably due to the decomposition of phytoplankton and other microflora. For those families who filtered their water before solar disinfection, it proved necessary to carry out cloth filtration three times before treatment, in order to reduce this problem. Around half of the bottles were lost or damaged over the year-long implementation period; however, laboratory tests also showed that while the remaining containers were often badly scratched by sand and grit, they were still able to provide effective disinfection, even after a year of regular use. Several users commented that the 1-liter bottles supplied by the project were too small, and should be replaced by larger containers (e.g. 2-liter or 5-liter bottles). In addition, several villagers commented that because the containers were given entirely free of charge, they were not held in such high regard as they would have been if a small charge had been levied. Any follow-up work should investigate the idea of charging a nominal fee for the container and reflector, in order to increase its worth in the eyes of the end-users. Similar conclusions have been reached for other small-scale water treatment systems (UNDP-World Bank Water and Sanitation Program 1999). Children were often found to be the most enthusiastic adopters of solar water treatment, taking responsibility for laying out the bottles each day, and then making use of the bottles at school. More recently, youth groups have been formed in both of the villages, and these have considerable promise for the continued implementation of solar water treatment. In hindsight, the use of a male researcher based outside the village created a barrier to communication with the women of each household, as face-to-face discussions could only be held in the presence of a village elder. A better strategy would be to work through a female worker sited within the village as part of a larger health awareness program, though this was outside the scope and funding of our project. Field trials in rural Rajasthan showed a measurable reduction in the incidence of gastroenteritis and diarrhea in a case-controlled trial over a 1-year period, demonstrating that solar disinfection can enable such households to widen their sources of treated drinking water. The historical record of the use of sunlight for the traditional ceremonial purification of drinking water should assist its wider acceptance as a practical approach to water treatment in rural Acra, A., Y. Karahagopian and Z. Raffoul. 1980. Water disinfection by solar radiation. Lancet II:1257-1258. UNDP-World Bank Water and Sanitation Program. 1999. Willing to pay but unwilling to charge. South Asia Field Note. Patwardhan., A. R.1990. Our water our life. Reed, R. H. 1997. Sunshine and fresh air: A practical approach to combat waterborne disease. Waterlines 15:27-29. Tandon, P., S. Chhibber, and R. H. Reed. 2005. Inactivation of Escherichia coli and coliform bacteria in traditional brass and earthenware water storage vessels. Antonie van Leeuwenhoek 88:35-48. |
|||||||||
 |
As this photograph shows, women may drink surface water directly from a talab, using cupped hands to drink the water through the mesh of their headscarf veil ("dupatta"). Brightly coloured dupattas and saris of pink, orange and red are typical of this part of Rajasthan. Water collection vessels made of iron and brass are also visible, alongside a plastic jerry can. |
||||||||
 |
Figure 7a shows the village tanka in Tulesar Purohitan. A range of different types of metal vessels are visible, including iron pitchers in the forground, with stainless steel and brass pitchers in the background. |
||||||||
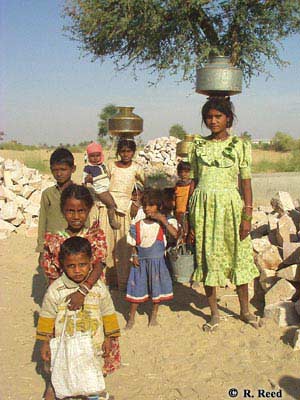 |
Figure 7b shows children carrying water using steel and brass pitchers - only the poorest families use earthernware pitchers for carrying water, as they are easily broken. In the villages used in this field study, water is carried only a short distance (typically less than 500 meters [~1/3 mi]), whereas in the interior of Rajasthan it may be several kilometers or more to the nearest water supply.
|
||||||||
 |
Here, a villager stirs fine sand ("balu mitti") into a bucket of turbid surface water – on settling, the sand will remove some of the particulates, thereby reducing the turbidity. |
||||||||
|
|
|||||||||
|
|
|||||||||